
A tongue tie is a tight, short, and/or thick string of tissue under the tongue that restricts movement and creates a postural and functional issue. Due to a lack of education in conventional dental and medical training, they are often misdiagnosed or misunderstood. Tongue ties can be divided into 2 categories: an anterior tongue tie that is an easily visible restrictive attachment at the tip of the tongue, and a posterior (submucosal) tongue tie that is a deeper fascial restriction lying under the tissue surface. It is estimated that anterior tongue ties occur in 4 to 10% of the general population, and a recent study by Marchesan and Martinelli concludes that posterior tongue ties occur in as many as 32.5% of infants.
Throughout our body, we have connective tissue networks that are responsible for “keeping our house in order”. These fascial tissue networks interconnect and support our muscles and organs throughout our body. When fascial tissue has the appropriate flexibility, muscles can work freely in their full range of motion. When a segment of the fascial tissue is tight and restrictive, it can limit muscle range of motion and result in tension.
In the oral cavity, fascial restrictions can occur in the frena, which are the lines of tissue connection of the tongue, lips, and cheeks. The lingual frenum, the labial frena, and the buccal frena. The lingual frenum is the top of the deep front line fascial chain that runs from our tongue to our toes.
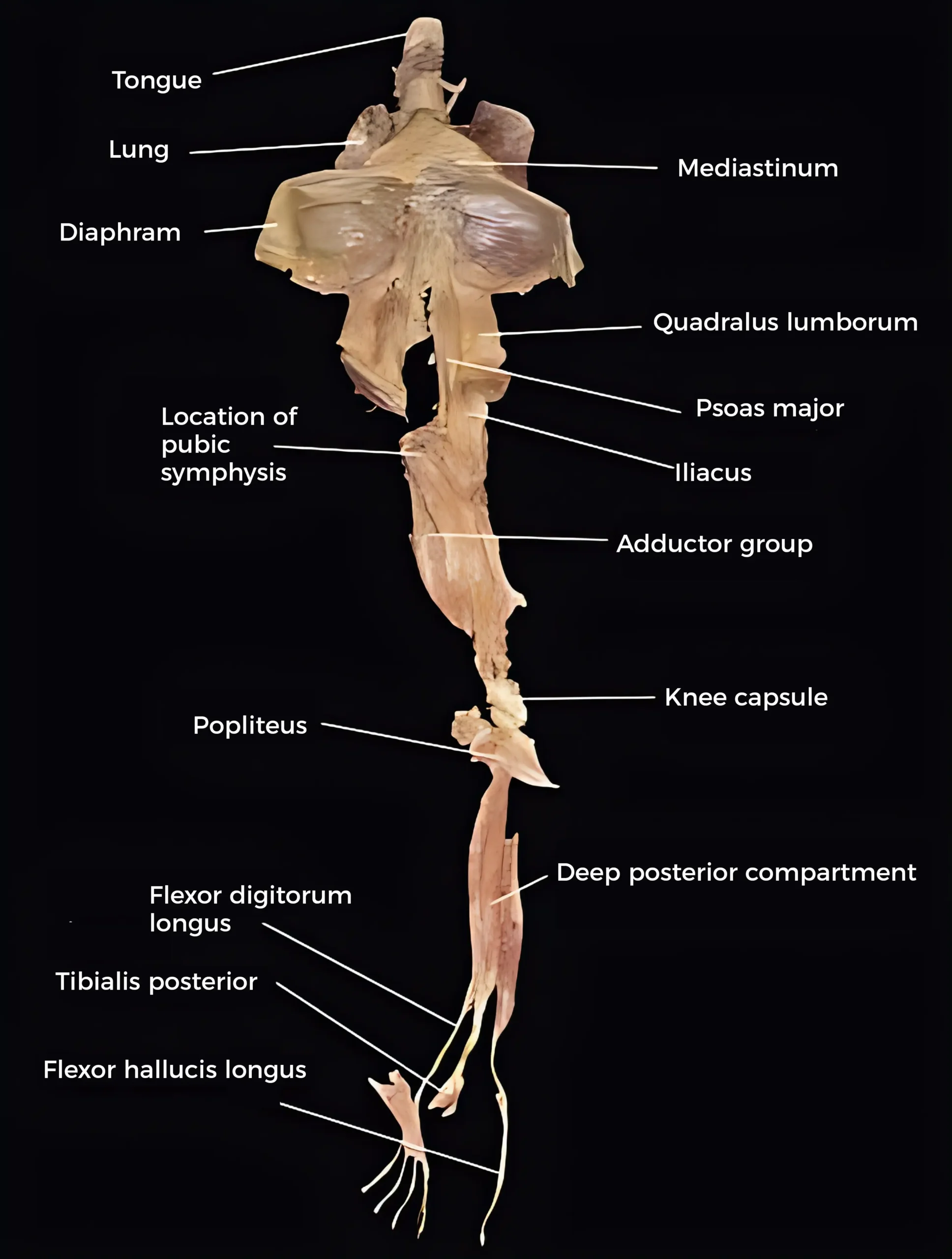
Curiously yet understandably, a tongue tie can sometimes be the root culprit behind something seemingly as far away as toe walking. When there is a restrictive attachment of the tongue, surrounding tongue and neck muscles have limits to their function, and we often see related myofascial tension arising closer to the source in the neck and shoulders. However, tension can result anywhere down the fascial chain from the head and shoulders to the toes.
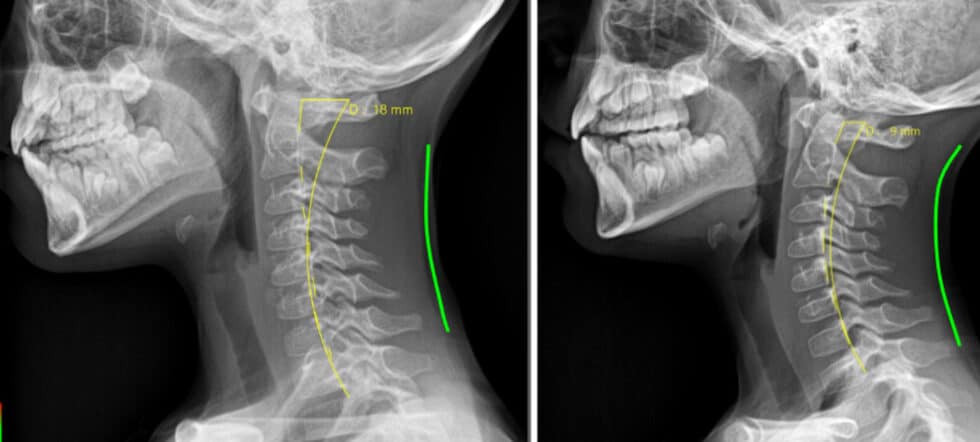
These images are of a child who presented with toe walking that was not resolving with typical bodywork protocols. His provider recognized a tongue tie and sent him here for tongue tie release with oral myofunctional therapy. These photos are 3 months apart. During that window, we treated the child with 2 months of oral myofunctional therapy and a functional tongue tie release with our Lightscalpel CO2 laser. The second image was just a few days after the tongue tie release procedure, where the patient not only showed resolution of toe walking, but also showed a return to healthy curvature of the cervical vertebrae with release of head and neck tension. It is important to state that success is dependent on a collaborative team approach that addresses not only the restriction of the tongue tie, but also addresses the compromised oral function and the surrounding muscle and fascial (myofascial) tension that is associated with it.
It is important to realize that everyone has tongue, lip, and cheek frenal attachments. Only when they are restrictive and affecting function and/or proper posture are they a problem that warrants treatment- a thorough assessment is necessary for this. The term tethered oral tissues collectively refers to tongue ties, lip ties, and buccal (cheek) ties.
For the line of connective tissue under the tongue to qualify as a tongue tie, it must have a functional impact on nursing, speech, feeding, or sleep.
Functional impacts for an infant:
- Painful/prolonged nursing
- “Clicking” and failure to maintain suction of latch
- Reflux and excessive spit up
- Gassiness
- Poor stimulation of maternal milk production
- Difficulty with weight gain
- Food aversions, gagging with the introduction of solid food
Functional impacts for ties remaining into childhood and adulthood:
- Speech delays and stuttering, along with troubles making certain sounds (often L, S, Z, SH, R, TH)
- Sleep impacts of a tongue tie can begin in infancy. A tongue tie does not allow the tongue to rest properly up and forward in the palate, and the resultant low and back resting tongue posture allows the base of the tongue to fall back into the airway and restrict airflow. Associated mouth breathing during sleep further disrupts proper airflow as the lower jaw drops down and back to impede the airway.
- Soft tissue imbalance from open mouth posture that often occurs with a tongue tie can lead to structural and functional changes in the jaw, face, and airway. These anatomical changes to the craniofacial and respiratory complex can impact TMJ (jaw joint) and sleep health throughout life.
- A dysfunctional swallow, with the tongue thrusting forward or laterally rather than the appropriate up and back tongue to palate swallow can exacerbate the structural changes of the jaw, face and airway. In some people, this inappropriate swallow can contribute to digestive problems from swallowed air or from a lack of vagus nerve stimulation of the palatoglossus muscle along the soft palate.
- Compensatory pain or dysfunction elsewhere in the myofascial (muscle and connective tissue) complex. This is commonly chronic head/neck/shoulder pain. It could be migraines or TMJ associated pain from parafunctional muscle activity grinding or clenching the teeth to get the tongue out of the airway during sleep. As seen above, it could also be something at the other end of the body like toe walking.
I encourage you to learn more about effects of tethered oral tissues, or “ties”, and about the procedure to release them on our services page https://stg-apexdental-staging.kinsta.cloud/tongue-tie-release/
Why the increase in ties? What is causing these restrictions? The role of genetics and epigenetics, Vitamin A, MTHFR, and folic acid.
I am a big “why” person. I don’t take things at face value. If I encounter an issue, I want to know “why”. Tethered oral tissues have been a known medical issue for many years. The condition of a tongue tie was given its official name “ankyloglossia” in the medical literature in the 1960s. Tongue ties were around long before that (albeit much less common than current times), but this was the time period that they gained more attention in the medical community due to their functional effects. With all of the research that I’ve done on the subject, there seems to be a definite genetic (hereditary) component which explains the long standing yet much less common history of tethered oral tissues, as well as a strong epigenetic (environmental) component which explains the sharp rise in incidence that we see in current times.
Fetal development is a complex phenomenon. In early development, many structures have connections that will not remain at birth (webbing of the fingers, attachment of the tongue to the floor of the mouth). Most babies are not born with webbed fingers (syndactyly) because the flaps of skin between the fingers are removed by a process of cell death called apoptosis. Around the 13th week in the womb, fetal tongue formation is completed with apoptosis of the extra flap of tissue under the tongue. This is crucial because it allows the tongue to posture high in the palate to apply passive pressure to grow the palate to an appropriate broad form. Without this step, the tongue will rest low which will pull the mandible down and back to a more recessed position and the palate will develop a high vault with coincident more narrow maxilla.
Studies published in the NIH’s National LIbrary of Medicine PubMed database, dating back to the 80’s, have isolated genetic mutations that have strong association with ankyloglossia (tongue tie). Research has found an isolated X-chromosome defect linked to both cleft palate and ankyloglossia . MTHFR gene mutations have also been isolated in higher risk of ankyloglossia. MTHFR gene mutations affect the ability to methylate folate into its usable form.
This is the perfect transition to epigenetic factors. Just because a genetic factor is present, doesn’t mean that it will cause an issue every time in the same way and to the same degree in everyone. Environmental (epigenetic) factors affect gene expression. Let’s look at some of the epigenetic factors reliably linked to tongue ties, then we’ll call it a day.
- Vitamin A deficiency. Vitamin A is a fat soluble vitamin known to activate genes for tissue apoptosis (cell death). Webbed digits (syndactyly) have been linked to vitamin A deficiency and vitamin A receptor mutations. Tongue tie and other tethered oral tissues are also a lack of apoptosis “cell death” of those tissue connections in early fetal development.
- Vitamin D and Vitamin K2 deficiency. Not only are these 2 fat soluble vitamins very important in fetal bone and hard tissue formation, they can also influence cell apoptosis to remove the early fetal tight tissue connections of the tongue and other structures.
- Synthetic Folic Acid build up. Usable methylated folate (B9) is indeed essential to proper fetal development, and efforts made in the 90s aimed to prevent the neural tube birth defects associated with its deficiency. Prenatal supplementation of synthetic folic acid began at that time. Synthetic folic acid was also added to much of the processed food supply through “fortified” flour and grains.The current CDC recommended dose for pregnant women is 400 micrograms of folic acid. In the typical “more must be better” approach, current prenatal vitamins contain 800 to 1000 mcg of folic acid, double the recommended dose. If you now consider the added folic acid exposure from fortified grains that are in nearly every processed food, that’s quite an excess of folic acid! Neural tube formation occurs in the first 4 weeks of pregnancy, which is a reason that prenatal supplementation is recommended to start prior to conception. Now we have a lot of folic acid (even more for moms with an MTHFR gene mutation that don’t properly convert folic acid to methyl folate) that helps with neural tube formation, but may also contribute to more amped up midline connective tissue formation. There is an interesting 2020 observational study published and available on PubMed that reports a significantly higher incidence of infants with ankyloglossia (tongue tie) in those mothers who supplemented with folic acid “on a regular basis” (54%) compared to a control group (25%). The incidence was much less significant for those who reported a less regular intake of folic acid before and during pregnancy.
As with everything, it is important to realize and acknowledge that multiple factors are always at play. The more that we can understand involved factors, the more that we can understand the prevalence of, as well as the prevention and treatment of, a condition. I encourage you to get nerdy and spend time on the NIH’s National Library of Medicine website, PubMed, and dive into things on your own.
✌️
